

Psychotropic Shooter
SSRIs linked to school shootings

There is no modern phenomenon more disturbing than school shootings. They are increasing in prevalence and severity over the last 20 year. Why?
Some postulate it’s the easy access to guns. Others argue it’s the increased mental illness. SSRIs have become one of the primary targets for those trying to solve this problem.
There are many sites like this one who claim the majority of school shooters are on psychotropic drugs like SSRIs.
In this article, we’ll examine what SSRIs are, how they supposedly work, and investigate any link between SSRIs and school shootings.
SSRIs are currently the most common antidepressant on the market. Before they were invented, drugs like monoamine oxidase inhibitors and tricyclic antidepressants were the major drugs prescribed, along with benzodiazepines. These drugs had horrible side effects, so Big Pharma went looking for alternatives.
SSRIs have been around officially since the late 1980s, when Eli Lilly and Company got Fluoxetine approved for use in depression. They hit the gold mine and reached over $2 billion per year worldwide with $350 million from the USA. In 2001 they lost the patent and SSRIs flooded the market.
Now SSRIs are everywhere. Depression is the most common psychiatric disorder in the world by a wide margin. These drugs are given out like candy.
SSRI stands for selective serotonin reuptake inhibitor. These drugs work by inhibiting reuptake of serotonin in presynaptic neurons in the brain. I have attached the image below for those interested.
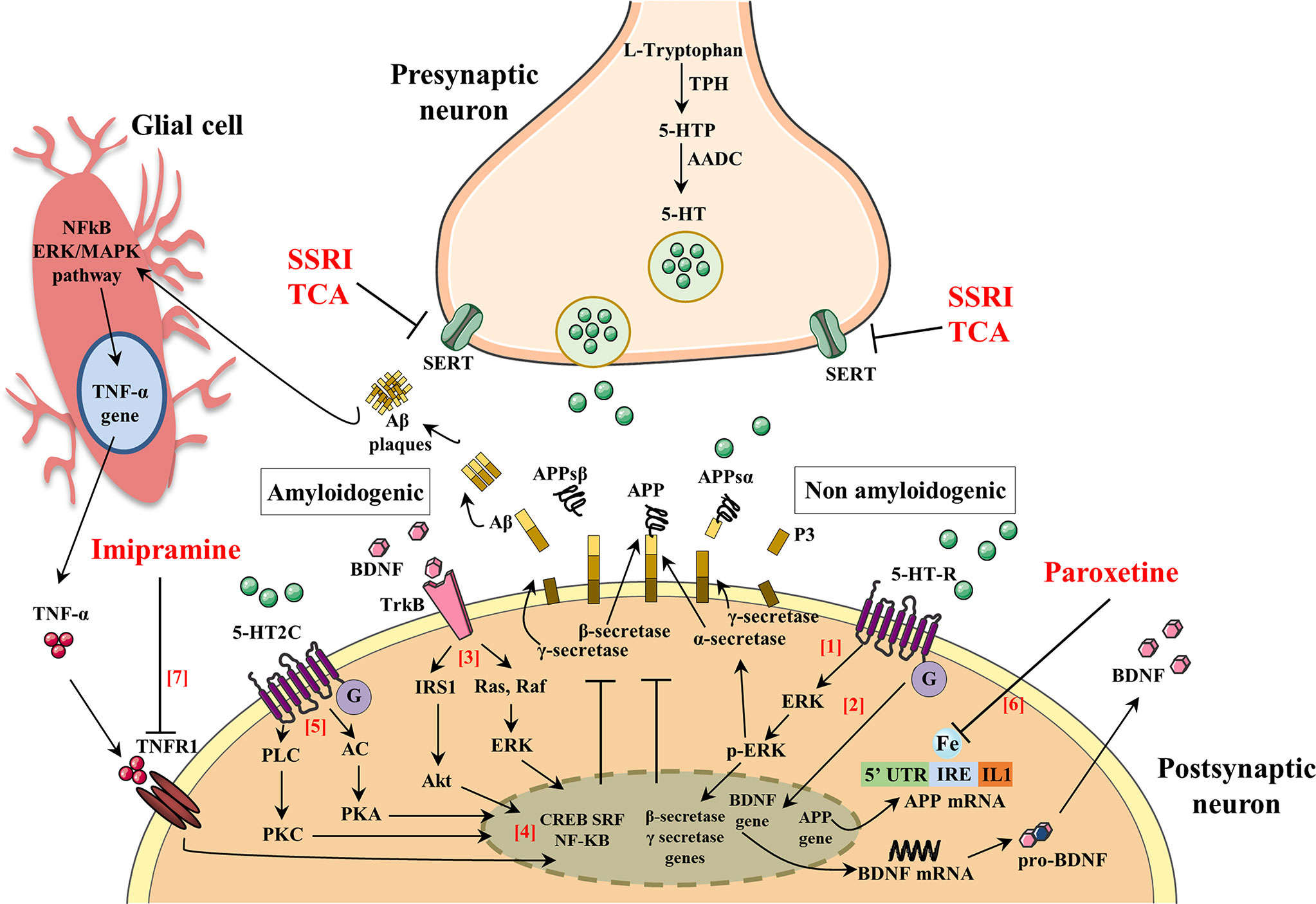
In plain language, when neurons in the brain release serotonin it binds to other neurons. The serotonin is then taken back up into the neuron and recycled. SSRIs prevent the neurons from reabsorbing serotonin making more of it available to activate neurons in the brain.
This was sold as a breakthrough discovery. These drugs were marketed as a supplement of serotonin for those who were deficient - those with depression.
Anyone paying attention knew the “serotonin hypothesis of depression” was wrong the whole time. It was predated by the norepinephrine hypothesis, which was also wrong. Turns out it’s also not dopamine. A large systemic review of the serotonin theory of depression was released in 2022. This opened the eyes of millions, although some still have their head buried.
The reality is, SSRIs were a happy accident for Eli Lilly. Big Pharma had tried targeting monoamines (MAO inhibitors), norepinephrine didn’t work (tricyclic antidepressants), and dopamine was the primary target for schizophrenia. Serotonin was the only target left.
Big Pharma’s search for the great white whale was bound to be successful with enough money and endless opportunities. Their marketing genius made its success a guarantee.
An interesting aspect of SSRIs which is common to many medications is the idea of tolerance. Many people start with a small dose and find themselves increasing their dose over time. Eventually they have to add another drug, and another, and so on.
The reason for this is well understood. When the neuron is flooded with serotonin it doesn’t like it. It down regulates and reabsorbs some of the receptors to prevent itself from being stimulated so much. That means you have to take more of the drug to maintain the same level of functionality.
This phenomenon also makes it very difficult to get off these meds. If you cut the dose, your neurons freak out. It’s like skipping coffee for a few days after drinking 3 cups a day for 20 years.
The way these drugs are prescribed is nothing short of predatory. When someone complains of depression, they are offered an SSRI first. If the depression resolves the med is slowly tapered and stopped.
After a recurrence of depression the process is repeated except the person is kept on the SSRI for upwards of a year. Then they are tapered and stopped again.
If a person relapses a second time, they are given the drug infinitely - usually forever. That is the jackpot for Big Pharma. They have a return customer for life without having to do anything.
Another issue with these medications is they are all different. Even though they all fall under the SSRI category, they have a slightly different mechanism of action. They have different additives. They are made by different companies with different quality controls. People react differently to all of them.
That means it’s basically guess and check. The doctor picks their preferred SSRI and tells the patient to take it for 3 months and let them know how they feel. If they aren’t feeling anything after 3 months, they increase the dose. Then again. Then maybe they try a different one and repeat the process.
This is a terrible system which is highly subjective. The results are not great.
So, what does all of this have to do with school shootings?
