

The Infamous Pop
Deciding if you need surgery for your ACL tear

We have all seen it. An athlete makes a sudden direction change, lands awkwardly, or maybe is just running in open field.
POP!
All of a sudden that leg goes limp. Pain ensures. The knee swells to the size of a grapefruit. It’s the ACL. There goes their season.
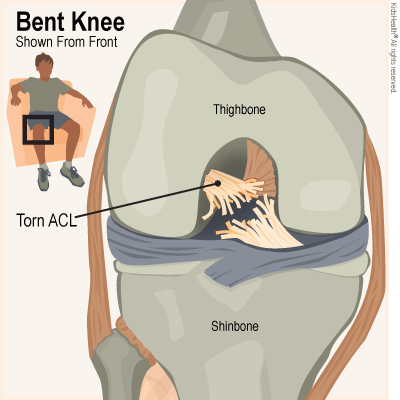
Maybe it’s happened to you. That wouldn’t be uncommon considering it’s one of the most common orthopedic injuries. Roughly 68 per 100,000 people tear their ACL yearly.
The first step in evaluating the knee is likely a trip to your primary care doctor. Most of them have enough basic understanding of ACL tears to identify a large tear. Smaller ones are harder to identify.
Due to insurance company requirements they usually have to start their diagnosis with a knee X-ray. Since it was already obvious you didn’t fracture your knee, this is a waste of time and money. With that done the PCP can usually send you to an Orthopedic surgeon and schedule an MRI.
MRI’s are far better at diagnosing ligament damage than an X-ray, and usually better than a CT scan (although CT scan does have some advantages). Results show a tear and will hopefully identify the severity.
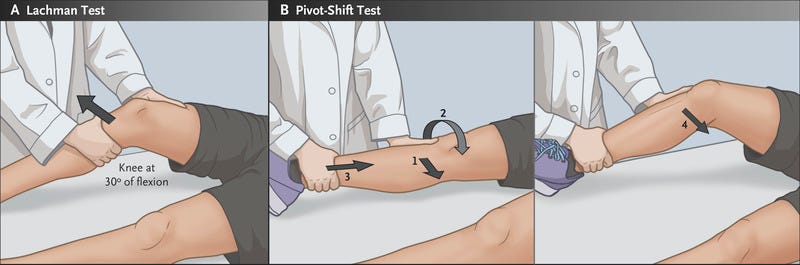
Now it’s time to see the surgeon. They may get their own MRI or CT scan in their office, making your first one a waste of time (and money). They will examine the knee and perform a series of tests to confirm or identify which ligament is damaged. A skilled clinician can identify the damaged ligament reliably with tests like the Lachman, drawer test, McMurray, Thessaly, among others. They make their recommendations (usually surgery) and 6 weeks later you’re under the knife.
9 months after the surgery you’re back to whatever activity you want and can live your life as you wish. Until it happens to the other knee or worse, the same knee again.
This whole process realistically takes about a year from POP! to walk.
